
A focus on prevention: misshapen heads in newborns

Misshapen heads in newborns are a common concern.
Approximately 30% of newborns will either be born with or develop a misshapen head within the first few months of life.
2 main types of misshapen heads
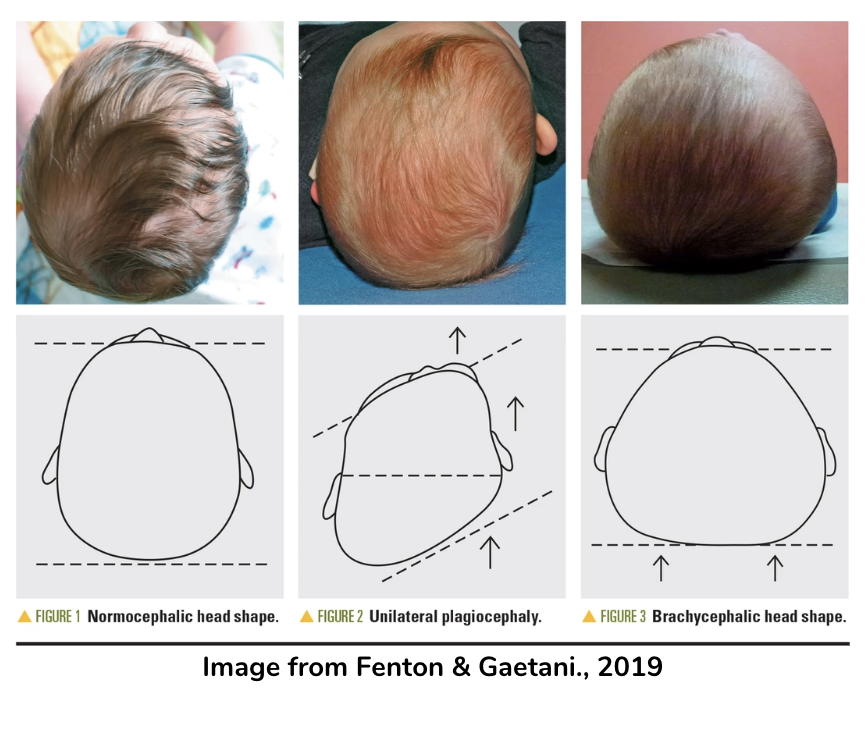
1. Positional Plagiocephaly
Flattening on one side of the back of the head. It can cause the ear to move forward and low and the forehead to bulge on the same side as the flattening. A parallelogram head shape can sometimes be seen when looking from the top.
2. Brachycephaly
Flattening on the back of the head on both sides. It can cause the back of the head or the distance between the ears to look wider.
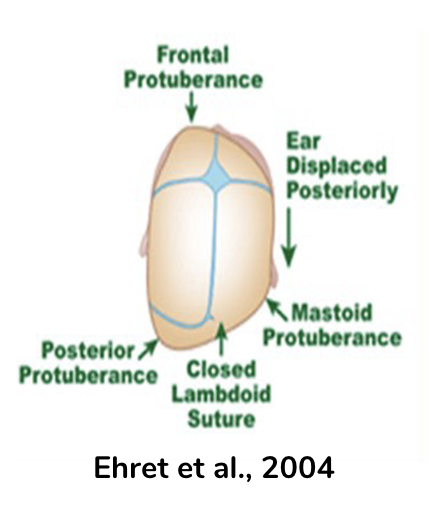
There is a 3rd type which requires urgent and specialised treatment called craniosynostosis. It occurs when the skull bones fuse together too early and can restrict brain growth. It has a trapezoid appearance when looking from above.
It is important that any misshapen heads be assessed by a health professional to be sure early fusion has not occurred. Early fusion requires intensive treatment and sometimes surgery.
Preventing misshappen heads
Follow these 5 evidence based strategies:
1. Sleep positions
Back to Sleep. Always place infants on their back to sleep. and follow safe sleep guidelines for prevention of Sudden Infant Death Syndrome (SIDS). This is NOT NEGOTIABLE.
- Turn your baby’s head each time you lay your baby down for a sleep and swap which side their head is turned at the start of each sleep. TIP: Place a peg or stroller clip on the cot or bassinet on the side you turn their head towards. Next time you lay them down you will know which side they were last on. You can turn their head to the other side and move the peg to keep track.
- Turn the cot or bassinet OR alternate which end of the bed their head is placed. Babies like to turn their head towards anything stimulating. Examples could be a door, light, furniture, you walking into the room, noise or anything stimulating.
2. Play positions & environment
Tummy Time
- Aim for tummy time at least 3 times a day. Try in each awake cycle.
- Start with 2 or 3 minutes at a time and increase as baby becomes more comfortable.
- Aim for 15-30 minutes in a 24 hour period by 7 weeks old and 80 minutes (1hr 20 minutes) by 4 months old.
- Safe to start from day 1 of life in healthy newborns.
How to do Tummy Time:
- Spread toys evenly from left to right in front of baby.
- Make noises, engage, use bright colorful and noisy toys on both sides and infront.

3. You can do tummy time on your chest when you are reclined, sitting up or laying down.

4. Add a rolled towel, wrap or blanket under babies chest. You can place a hand on their bottom to help stabilise them.

5. Superman on your legs.

6. Carrying in tummy time.
Sidelying

- Play in sidelying when supervised and supported when needed.
- Practice on both sides. If your baby likes to turn their head one way (for example the right), lay them on their opposite side (left side) for sidelying play.
- Use rolling to the side during nappy changes or when picking your baby up. Support your baby's head in the first 2-3 months of life.
Sitting to play

- Supported around the trunk and head as a newborn. This is usually seated on you in the first month of life.
- Independently or supported at the hips when head and trunk control have developed.
- Sitting in washing baskets or boxes with toys. This must be supervised and for short periods only.
- Independent sitting should be achieved by 9 months.
On the back
If all other positions are not tolerated and your baby needs to be more supported you can choose to have some play time on the back.
- Toys should be positioned on both the left and right sides of baby.
- If using a jungle gym or A-frame position hanging toys more to the sides rather than in the middle to encourage increased head movement and reaching
3. Carrying positions
A range of carrying positions encourages back, tummy and neck strength and motor development. Baby will want to look around more, encouraging neck movement and less pressure on their head. These photos give you some options to try.
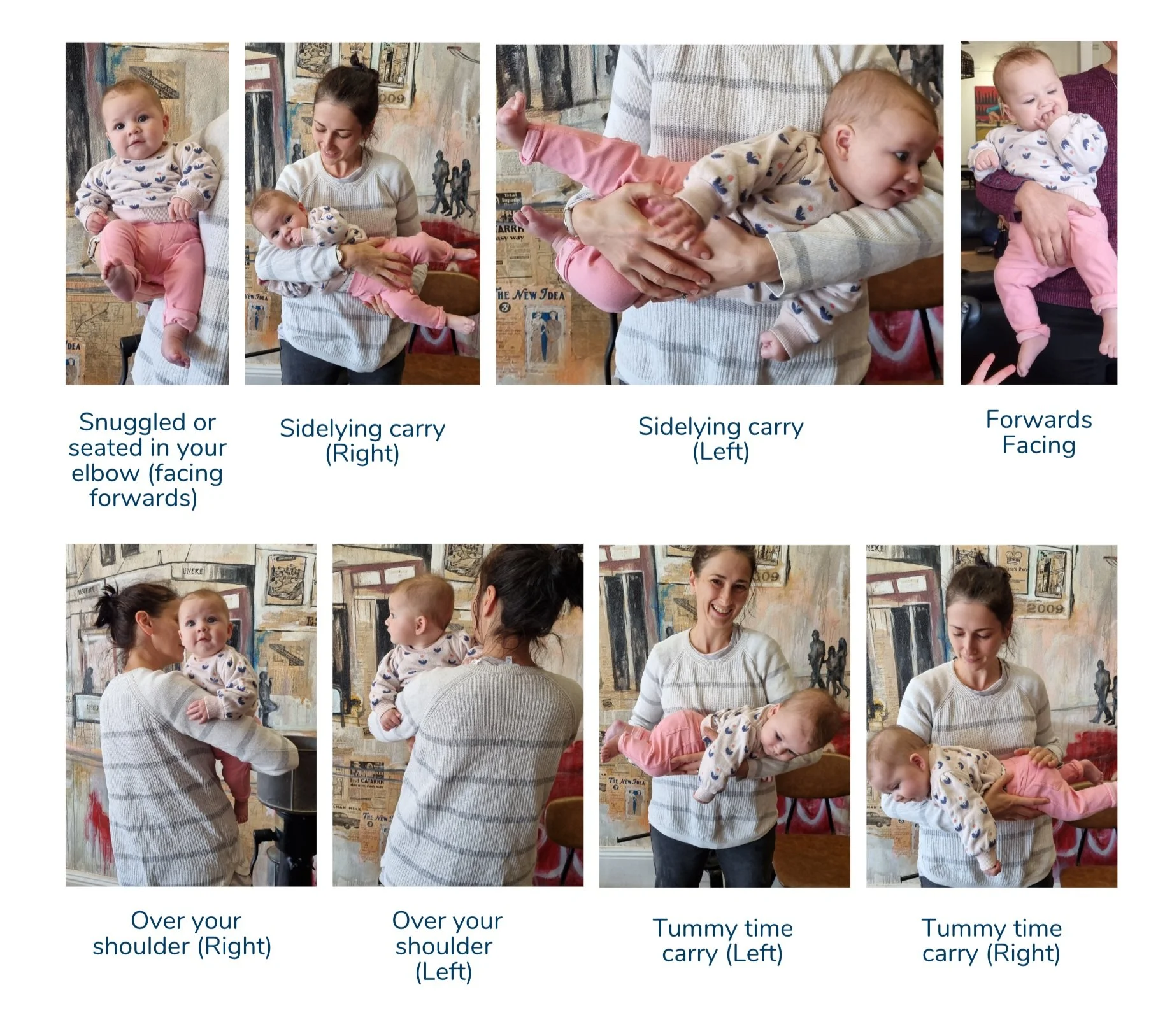
If your baby has not developed head and neck control, please support their head in all positions.

4. Alternate feeding sides
- Feed your baby from both sides.
- Breast fed babies should be offered sides on an alternating basis.
- If your baby is bottle fed, alternate which arm you hold them in for each feed.
This may also protect your body from overload.
5. Avoid containment
This means avoid placing your baby in”containers” or in other terms equipment that straps your baby in. This includes bouncers, rockers, swings, jolly jumpers, and sit in walkers. Car seats and capsules are essential for safety while travelling. They should not be used in the home as a sleeping aid or during awake play time.
Here are some facts about container use:

- More than 30 minutes in a containing device per day can limit motor development.
- More than 2 hours at a time in a capsule can be bad for spinal development.
- They limit baby’s ability to initiate movement.
- Babies recieve less feedback from their movement in containers.
- Using containers instead of floor play may impact learning and development.
When to act?
The answer is NOW. Whether or not your baby has a misshapen head, you can start the above strategies now, regardless of how young your infant is. If your baby was born prematurely (less than 36 weeks gestation), these strategies are still safe. Follow any advice given by your healthcare team first and if you are unsure ASK.
PREVENTION is easier than TREATMENT.
If your baby always looks to one side or has a small flattening on their head, and these strategies are not helping within 2-3 weeks, please seek personalised advice and an assessment from a Paediaitric Physiotherapist or a member of your healthcare team.
Disclaimer: This is general advice based on recent evidence. If you have any questions or concerns please seek support from a member of your healthcare team or contact us on 02 69257734 to discuss with one of our friendly Physiotherapists.
REFERENCES
Lennartsson, F., & Nordin, P. (2019). Nonsynostotic plagiocephaly: A child health care intervention in Skaraborg, Sweden. BMC Pediatrics, 19(1), 1–12. CINAHL Plus. https://doi.org/10.1186/s12887-019-1405-y
Leung, A., Mandrusiak, A., Watter, P., Gavranich, J., & Johnston, L. M. (2018). Impact of Parent Practices of Infant Positioning on Head Orientation Profile and Development of Positional Plagiocephaly in Healthy Term Infants. Physical & Occupational Therapy In Pediatrics, 38(1), 1–14. https://doi.org/10.1080/01942638.2017.1287811
Trottier, N., Hurtubise, K., Camden, C., Cloutier, W., & Gaboury, I. (2023). Barriers and facilitators influencing parental adherence to prevention strategies for deformational plagiocephaly: Results from a scoping review. Child: Care, Health and Development. 1-18. https://doi.org/10.1111/cch.13095
Hewitt, L., Kerr, E., Stanley, R. M., & Okely, A. D. (2020). Tummy Time and Infant Health Outcomes: A Systematic Review. Pediatrics,145(6) https://doi.org/10.1542/peds.2019-2168
Jennings, G. T., Sarbaugh, B. G., & Payne, N. S. (2005). Conveying the message about optimal infant positions. Physical and Occupational Therapy in Pediatrics, 25, 3-18,
Subscribe to our Newsletter
Receive the latest news and insights to your inbox. No fluff or spam.
By subscribing you agree with our Privacy Policy



Book Your Appointment
Take the first step towards moving better and feeling stronger. Book online or contact us direct to schedule your initial consultation.
